Jump to paragraph
Introduction
Parkinson’s disease is the most standard explanation for Parkinsonism and is the second most common neurodegenerative disease after Alzheimer’s disease. Identifying dopamine deficiency within the brains of individuals with and, therefore, the subsequent introduction of replacement therapy with levodopa represents a substantial success story within the treatment of neurodegenerative illness. However, there remain various severe management problems in paralysis agitans, particularly within the advanced stages of the condition. Parkinson’s disease is the second most common neurodegenerative disease, affecting 1% of the population over 65.
Parkinson’s disease is characterized by bradykinesia, rest tremor, rigidity, and, later within the disease course, postural instability. Neuronal loss in the brainstem (substantia nigra) leads to a profound dopamine deficiency in the striatum. That provides the rationale for dopaminergic replacement therapies. Depression is common in Parkinson’s disease. It is the primary determinant of quality of life and is often missed. The depression of paralysis agitans is often readily treated. Levodopa, including a dopa-decarboxylase inhibitor, remains the foremost potent oral treatment for paralysis agitans.
There is debate as to whether levodopa should be deferred in biologically young patients, in an attempt to delay the onset of motor complications. Several other drug treatments are available for the management of paralysis agitans. When given as adjunctive therapy, the primary aim of these agents is to smooth out motor fluctuations. End-of-dose deterioration and, therefore, the on-off phenomenon are motor complications synonymous with the utilization of levodopa, usually after various years.
Symptoms of Parkinson’s disease
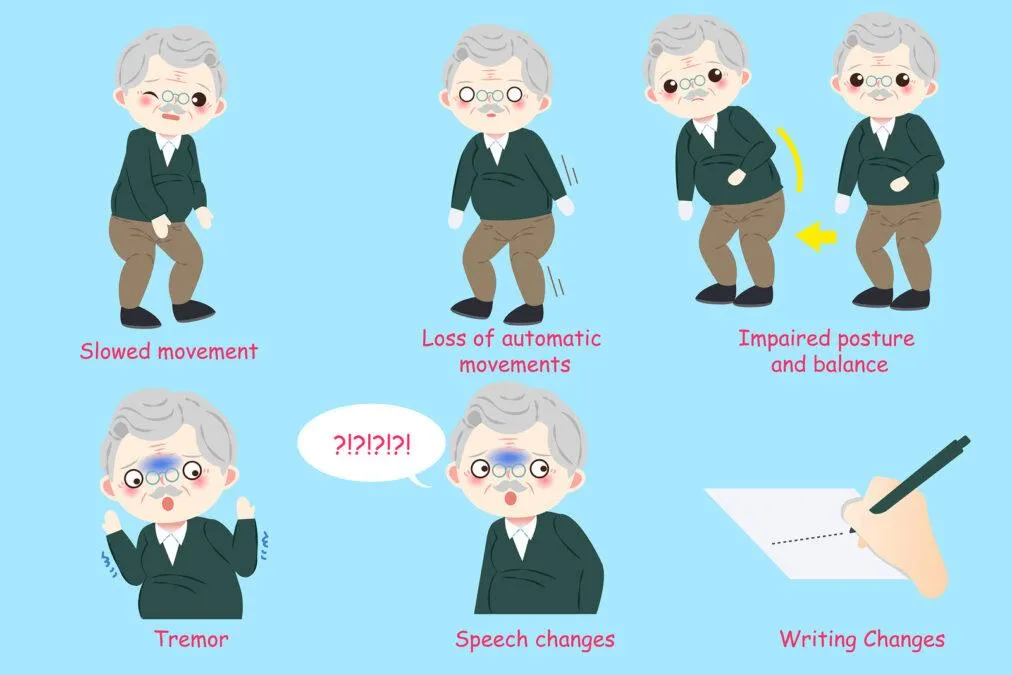
Some of the first symptoms of Parkinson’s can precede motor problems for several years. These earliest signs include:
- decreased ability to smell (anosmia)
- constipation
- small, cramped handwriting
- voice changes
- stooped posture
The four major motor problems seen are:
- tremor (shaking that occurs at rest)
- slow movements
- stiffness of arms, legs, and trunk
- problems with balance and tendency to fall
Secondary symptoms include:
- blank facial expression
- a tendency to get stuck when walking
- muffled, low-volume speech
- decreased blinking and swallowing
- a tendency to fall backward
Causes of Parkinson’s disease
The exact cause of Parkinson’s is unknown. It may have both genetic and environmental components. Some scientists think that viruses can trigger Parkinson’s as well.
Low levels of dopamine and norepinephrine, a substance that regulates dopamine, have been linked with Parkinson’s. Abnormal proteins called Lewy bodies have also been found in the brains of people with Parkinson’s. Scientists don’t know what role, if any, Lewy bodies play in the development of Parkinson’s.
While there’s no known cause, research has identified groups of people who are more likely to develop the condition. These include:
- Sex: Men are one and a half times more likely to get Parkinson’s than women.
- Race: Whites are more likely to get Parkinson’s than African Americans or Asians.
- Age: Parkinson’s usually appears between the ages of 50 and 60. It only occurs before the age of 40 in 5-10 percent of cases.
- Family history: People who have close family members with Parkinson’s disease are more likely to develop Parkinson’s disease, too.
- Toxins: Exposure to certain toxins may increase the risk of Parkinson’s disease.
- Head injury: People who experience head injuries may be more likely to develop Parkinson’s disease.
Stages OF Parkinson’s Disease

Parkinson’s disease is progressive diseases, and it is divided into different stages. Each stage explains the event of the illness and therefore, the symptoms a patient is experiencing. These stages increase in number because the disease increases in severity. It focuses almost entirely on motor symptoms.
People with Parkinson’s disease experience the disorder in several ways. Symptoms can range from mild to debilitating. Some individuals may transition smoothly between the five stages of the disease, while others may skip stages entirely. Some patients will spend years in Stage One with only a few symptoms. Others may experience a faster progression to the top stages.
Stage One: Symptoms affect just one side of your body.
The initial phase of Parkinson’s disease typically presents with mild symptoms. Some patients won’t even detect their symptoms within the earliest phases of this stage. In stage One, the common symptoms experienced are tremors and shaking limbs. Relations and friends may begin to note other symptoms, including tremor, poor posture, mask face, or loss of countenance.
Stage Two: Symptoms begin affecting movement on each side of your body.
Once the motor symptoms of Parkinson’s disease affect each side of the body, you’ve got progressed to Stage Two. you’ll begin having trouble walking and maintaining your balance while standing. You’ll also start noticing increasing difficulty performing once-easy physical tasks, like cleaning, dressing, or bathing. Still, most patients during this stage lead in everyday life with little interference from the disease.
During this stage of the disease, you’ll begin taking medication. The foremost common first treatment for Parkinson’s disease is dopamine agonists. This medication activates dopamine receptors, which make the neurotransmitters move more quickly.
Stage Three: Symptoms are more pronounced, but you’ll still function without assistance.
The third stage is taken into account moderate Parkinson’s disease. During this stage, you’ll experience apparent difficulty with walking, standing, and other physical movements. The symptoms can interfere with lifestyle. You’re more likely to fall, and your physical activities become far more difficult. However, most patients at this stage are still ready to maintain independence and wish little outside assistance.
Stage Four: Symptoms are severe and disabling, and you regularly need assistance to steer, stand, and move.
Stage Four Parkinson’s disease is usually called advanced Parkinson’s disease. People during this stage experience severe and debilitating symptoms. Motor symptoms, like rigidity and bradykinesia, are visible and challenging to beat. Most of the people in Stage Four aren’t ready to live alone. They have the help of a caregiver or home health aide to perform routine tasks.
Stage Five: Symptoms are the foremost severe and need you to be wheelchair-bound or bedridden.
The final stage of Parkinson’s disease is the most severe. you’ll not be ready to perform any physical movements without assistance. For that reason, you want to accept a caregiver or a facility that will provide one-on-one care.
Quality of life declines rapidly within the final stages of Parkinson’s disease. Additionally, to advanced motor symptoms, you’ll also begin experiencing greater speaking and memory issues, like Parkinson’s disease dementia. Incontinence issues become more common, and frequent infections may require hospitalization. At now, treatments and medicines provide little to no relief.
Whether you or a loved one is within the earliest or the later stages of Parkinson’s disease, remember that the condition isn’t fatal. Of course, older individuals with advanced-stage Parkinson’s disease may experience complications of the disease, which will be deadly. These complications include infections, pneumonia, falls, and choking.
Diagnosing Parkinson’s disease
There’s no specific test for diagnosing Parkinson’s. Diagnosis is formed supported health history, a physical and neurological exam, and a review of signs and symptoms.
Imaging tests, like a scan or MRI, could also be wont to rule out other conditions. A dopamine transporter (DAT) scan can also be used. While these tests don’t confirm Parkinson’s, they will help rule out other conditions and support the doctor’s diagnosis.
Medication
Several various drugs are often wont to treat Parkinson’s.
- Levodopa
Levodopa is the most typical treatment for Parkinson’s. It helps to replenish dopamine.
About 75 percent of cases answer levodopa, but not all symptoms are improved. Levodopa is usually given with carbidopa. Carbidopa delays the breakdown of levodopa, which successively increases the supply of levodopa at the barrier.
- Dopamine agonists
Dopamine agonists can imitate the action of dopamine within the brain. They’re less effective than levodopa, but they will be useful as bridge medications when levodopa is a smaller amount.
Drugs during this class include bromocriptine, pramipexole, and ropinirole.
- Anticholinergics
Anticholinergics are wont to block the parasympathetic systema nervosum. That will help with rigidity.
Benztropine (Cogentin) and trihexyphenidyl are anticholinergics wont to treat Parkinson’s.
- Amantadine (Symmetrel)
Amantadine (Symmetrel) is often used alongside carbidopa-levodopa. It’s a glutamate blocking drug (NMDA). It offers short-term relief for involuntary movements (dyskinesia), which will be a side effect of levodopa.
Diagnosing Parkinson’s disease
There’s no specific test for diagnosing Parkinson’s. Diagnosis is formed supported health history, a physical and neurological exam, and a review of signs and symptoms.
Imaging tests, like a scan or MRI, could also be wont to rule out other conditions. A dopamine transporter (DAT) scan can also be used. While these tests don’t confirm Parkinson’s, they will help rule out other conditions and support the doctor’s diagnosis.
SURGICAL PROCEDURES
There has been renewed interest in the use of neurosurgical techniques for the treatment of paralysis agitans. That has resulted not only from a recognition of the shortcomings of medical therapy currently available but also from an improved understanding of basal ganglia circuitry and better neuroimaging methods. The nucleus target is the current target of choice in most centers. Therefore, the number of published patient-years experience with this surgical approach has increased rapidly over the past decade.
Careful case selection is essential for all sorts of surgical intervention for Parkinson’s disease: older and fewer biologically fit patients, active cognitive or neuropsychiatric problems, and patients with a suboptimal levodopa response are generally considered poor surgical candidates.
NEUROPROTECTIVE THERAPY
Potential neuro defensive specialists that will slow illness movement are cell reinforcements, antiapoptotic operators, glutamate foes, intraparenchymal controlled glial-determined neurotrophic factor, coenzyme Q10, creatine, and calming drugs. The role of those agents remains to be established, however, and their use for therapeutic purposes isn’t indicated at this point. The likelihood that rasagiline features a protective effect was discussed earlier.
GENE THERAPY
Gene therapy for Parkinson’s disease has now been completed within the USA. All trials involved infusion into the striatum. The genes for glutaminic acid decarboxylase (GAD, to facilitate the synthesis of GABA, an inhibitory neurotransmitter), are infused into the nucleus to cause inhibition. After that, they are infused into the putamen to extend the metabolism of levodopa to dopamine. And for nurturing (a protein which will enhance the survival of dopaminergic neurons), infused into the putamen. All agents were deemed safe, and therefore the data suggested efficacy.
Exercise
Drugs and drugs wont to treat Parkinson’s disease۔
Parkinson’s often causes problems with daily activities. But elementary exercises and stretches may help you move around and walk more safely.
- To improve walking
- Walk carefully.
- Pace yourself — try not to move too quickly.
- Let your heel hit the floor first.
- Check your posture and stand up straight. That will help you to shuffle less.
- To avoid falling
- Don’t walk backward.
- Try not to carry things while walking.
- Try to avoid leaning and reaching.
- To turn around, make a U-turn. Don’t pivot on your feet.
Bonus video: What is Parkinson’s Disease?
FAQ’s
What is end-stage Parkinson’s?
When patients reach stage five – the ultimate stage of paralysis agitans – they will have severe posture issues in their back, neck, and hips. They’re going to require a wheelchair and should be bedridden. In the end-stage of paralysis agitans, patients also will often experience non-motor symptoms.
Do all Parkinson’s patients develop dementia?
An estimated 50 to 80 percent of these with Parkinson’s eventually experience dementia as their disease progresses. Some studies have reported that the typical time from Parkinson’s to developing dementia is about ten years. Hallucinations during a one that doesn’t yet produce other dementia symptoms.
Does stress cause Parkinson’s?
Research suggests that stressful life events may increase the danger of paralysis agitans. Additionally, animal studies indicate that stress damages dopamine cells, leading to more severe parkinsonian symptoms. In humans, acute stress can worsen motor symptoms, including bradykinesia, freezing, and tremor.
Is CBD oil effective in Parkinson’s?
Some studies suggest CBD may have some positive effects, especially when it involves nonmotor symptoms, like depression, anxiety, and sleep disorders. Ways to use CBD for Parkinson’s
If you’re a beginner with CBD, you’ll be interested in the most uncomplicated thanks to taking it if you’ve got Parkinson’s disease.
CBD is out there within the following forms:
Oils and tinctures. As liquids, these sorts of CBD are often swallowed or absorbed sublingually (under the tongue). That could be an honest option if you’ve got difficulty swallowing pills or chewing gummies.
Lotions and creams. The consequences of CBD-infused lotions and creams can take several hours to develop, but could also be useful to treat pain or stiffness in hands and joints.
Capsules and pills. You’ll experience a delay in effects if you’re taking CBD during a capsule or pill, but this type could also be ideal for people with tremors that prevent them from adequately doing a liquid.
What is the best exercise for Parkinson’s disease?
Biking, running, Tai chi, yoga, Pilates, move, weight preparing, non-contact boxing, qi gong, and the sky is the limit from there — all effects affect PD manifestations. There’s no “activity solution” that is directly for every individual with PD. The sort of exercise you are doing depends on your symptoms and challenges.
How long can an individual accept Parkinson’s disease?
On average, people with Parkinson’s can expect to measure almost as long as those with the disorder. While the disease itself isn’t fatal, related complications can reduce anticipation by 1 to 2 years.
How Parkinson’s disease is diagnosed?
Diagnosis. No specific test exists to diagnose paralysis agitans. Your doctor trained in systema nervosum conditions (neurologist) will diagnose paralysis agitans supported your medical record, a review of your signs and symptoms, and a neurological and physical examination.
What can mimic Parkinson’s disease?
Progressive supranuclear palsy (PSP) may be a disease that mimics PD, particularly early in its course, but comes with additional distinctive signs and symptoms. Those with PSP also often have problems with swallowing (dysphagia), difficulty producing speech (dysarthria), sleep problems, and thinking problems.
What vitamins are good for Parkinson’s disease?
Key dietary factors discussed below include reducing toxic load, reducing homocysteine with vitamin Bc, vitamins B12 and B6, zinc and tri-methyl-glycine (TMG), and increasing Omega 3 fats, vitamin D, and Magnesium. Read on for more information on paralysis agitans and the way it is often influenced by nutrition.
How is life with Parkinson’s disease?
Parkinson’s disease (PD) is challenging to measure because it causes progressive changes to motor function, also as many other non-motor symptoms, including depression, sleep problems, pain, and cognitive dysfunction.
Reference:
Roger Walker Clinical Pharmacology